

When it comes to the female body, it’s safe to say how we feel, look, think and perceive things can change dramatically over the course of our cycle. Our body’s hormones control everything from our metabolic function to our pain threshold, to how we eat, and even to how much training we can tolerate. Up to 80% of women report symptoms such as acne, bloating, fatigue, and mood changes in the couple of weeks leading up to menstruation (1,2). Understanding what happens throughout the phases of your cycle can give you valuable insight into why you feel strong and powerful during one phase to weak and weepy in the other.
Using an App such as MyCalendar allows you to track your cycle and collect data over time, which will help you to determine the average duration of your cycle and when it's next expected.
The phases of your menstrual cycle
There are four phases of the menstrual cycle. They are the:
- menstruation,
- follicular,
- ovulation, and
- the luteal phase.
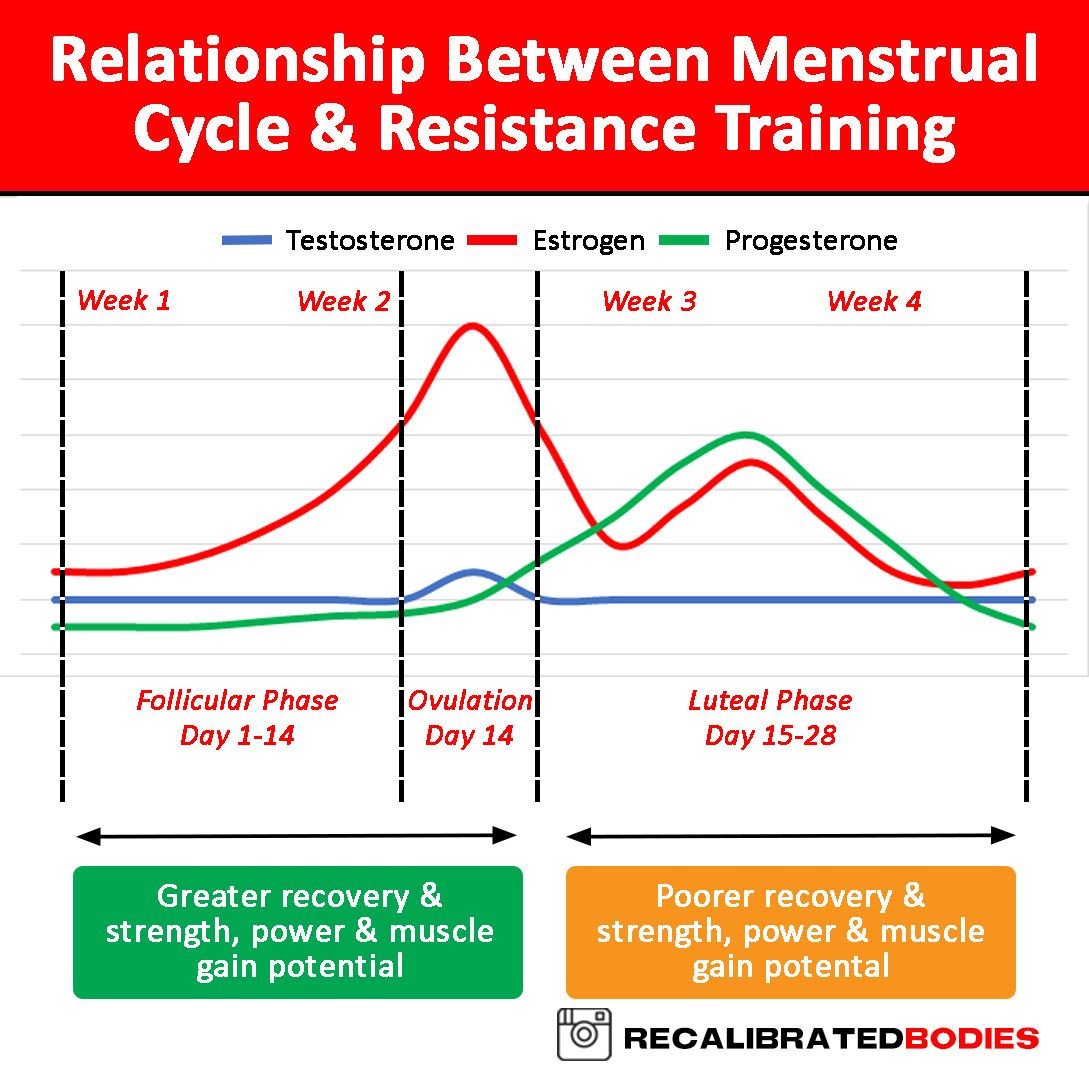
Your menstrual cycle starts with the menstrual phase; i.e. when you get your period. Next is the follicular phase, which starts on the first day of your period (there is some overlap with the menstrual phase), lasts about 14 days, and ends when you ovulate. From here, we move into the ovulation phase, which only lasts a day or two. After the ovulation phase, we then move into the dreaded luteal phase, lasting again about 14 days and ending on day 28 - this is where things can get nasty! If you do experience PMS symptoms, it’s in the luteal phase that they will become apparent. Menstruation will soon start and the cycle begins all over again. A normal menstrual cycle can be anywhere between 28 and 35 days long. Its duration can also differ on a month-to-month basis. Using an App such as MyCalendar allows you to track your cycle and collect data over time, which will help you to determine the average duration of your cycle and when it's next expected, as it will be different for us all. It can also be useful to measure your body temperature to estimate your menstrual cycle phase. Body temperature tends to spike by at least 0.3° C around ovulation - the midpoint of your cycle between the follicular and luteal phase (3).
Training more frequently in the first two weeks, from menstruation to ovulation, has been shown to be more beneficial to gain power, strength and lean body mass, compared to the last two weeks.
Follicular Phase
This phase is the fun phase when you can really push the boundaries with training. Oestrogen increases at this stage, which is anti-catabolic and aids in muscle recovery (4), which means a noted increase in strength and muscle growth is often observed (5). Training more frequently in the first two weeks, from menstruation to ovulation, has been shown to be more beneficial to gain power, strength, and lean body mass, compared to the last two weeks (6). Your pain threshold is increased, endurance levels are augmented, and your insulin sensitivity is increased so your body burns through muscle glycogen like an out-of-control furnace to fuel your training. When the body is more insulin sensitive, you require less insulin to keep blood glucose levels in the normal range and to keep your body’s cells supplied with glucose. Consequently, carbohydrates are used more efficiently (7). Simply put; focus on strength, interval, power, and hypertrophy-based training and remember, it’s definitely not a time to have carb-phobia!
This phase is when you turn into superwoman and is a great time to test for new PRs. Studies have shown as much as an 11% increase in both quad and hamstring strength in this time!
Ovulation Phase
Ovulation is characterised by a sharp increase in all hormones, including testosterone (8). This phase is when you turn into superwoman and is a great time to test for new PRs. Studies have shown as much as an 11% increase in both quad and hamstring strength in this time (9)! However, as oestrogen is at its highest, there is an increased risk of injury as oestrogen can affect collagen metabolism and influence your neuromuscular control (10). Therefore, it’s extremely important to keep your exercise technique on point to reduce the risk of injury while you’re pushing heavier weight. In good news, your metabolism is starting to increase, so it is normal for your appetite to increase with it - compared to the decrease in Basal Metabolic Rate (BMR) during the previous follicular phase (11). It’s also important to note that Mittelschmerz (German for middle-pain) may present in some ladies, which is characterised by dull cramp-like pain on one side of the lower abdomen (12). Lastly – and the big one for those trying to lose body fat - water retention and bloating can also present, which is important to remember as many mistake this gain in body weight as fat gain. Nope, it’s just your hormones! Arming yourself with such knowledge will keep panic at bay if this happens to you.
During this phase, it is a good idea to opt for lower-intensity cardio over interval training, and lower-intensity, higher-rep resistance training.
Luteal Phase
This is when the PMS symptoms kick in and things can head south. The normal luteal phase length from ovulation to menstruation ranges from 11 to 17 days with most luteal phases lasting 12 to 14 days (13). Your body experiences an increase in body temperature and water retention (1), reduced performance (14), and a metabolic increase of about 8% (15). Serotonin - your feel-good hormone - is lowered, which is why your mood is off. You’re snappy at everyone and you’re craving sugar. This is your body’s natural mechanism to try and increase serotonin levels from carbohydrates (16), as well as the result of falling oestrogen and progesterone levels. As a result, your body relies on fats more as a fuel source as opposed to muscle glycogen, as insulin sensitivity is at its lowest (7). During this phase, it is a good idea to opt for lower intensity cardio over interval training, and lower-intensity, higher rep resistance training (no convincing needed when everything feels like a tonne of bricks!). It's also a good idea to increase tryptophan-rich foods such as turkey and seeds - a precursor to serotonin - which may help spike serotonin production in the body.
## Menstrual Phase When menstruation begins, PMS symptoms tend to decrease, although cramping in the abdomen, lower back, and upper thighs can actually increase. This is when we transition into that ‘time of the month’ and your body feels like it’s returning to normal. Body temperature reduces, water retention starts to pass, energy begins to return, performance increases, fatigability reduces, and insulin sensitivity starts to increase again - good news for carb lovers! As the follicular phase approaches again, exercise intensity will naturally tend to increase.
Conclusion
With knowledge comes power. Learning what’s happening with your body’s hormones throughout our cycle gives us girls the ability to take advantage of certain times to train at certain intensities. The ovulation phase is the best time to train with the highest intensity (albeit it's a small window of opportunity lasting only a day or two), whilst the luteal phase is the worst time to try and train at max intensity, and lower intensity forms of training may suit you better. The luteal phase is also the time to be sceptical of your scale readings and body measurements, as this is the time you're likely to hold more water weight and bloat. It can be so disheartening to feel tight and strong one week, to watery and weak the next. Now that you know why this occurs, however, you can relax about the fluctuations on the scales, body measurements, progress pictures, and training performance you may experience - it’s all normal! Yes, it's all the joys of being a lady!
References
- Biggs W and Demuth R. Premenstrual syndrome and premenstrual dysphoric disorder. American Family Physician 84: 918–24, 2011.
- Barclift S. Premenstrual syndrome (PMS) fact sheet. Office on Women's Health, USA, 2014.
- Mouzon J, Testart J, LeFevre B, Pouly JL and Frydman R. Time relationships between basal body temperature and ovulation or plasma progestins. Fertility and Sterility 41: 254-59, 1984.
- Brown M. Estrogen Effects on skeletal muscle, Integrative Biology of Women’s Health: 35-51, 2013.
- Sung E, Han A, Hinrichs A, Vorgerd M, Manchado C and Platen P. Effects of follicular versus luteal phase-based strength training in young women. Springer Plus 3: 668, 2014.
- Wikström-Frisén L, Boraxbekk CJ and Henriksson-Larsén K. Effects on power, strength and lean body mass of menstrual/oral contraceptive cycle based resistance training. J Sports Med Phys Fitness. 57: 43-52, 2017.
- D'Eon T, Sharof C, Chipkin S, Grow D, Ruby B and Braun B. Regulation of exercise carbohydrate metabolism by estrogen and progesterone in women. American Journal of Physiology. 283 (5). 2002.
- Howard J and Samuels Y. Serum Androstenedione and Testosterone Levels During the Menstrual Cycle. Journal of Clinical Endocrinology & Metabolism. 36 (3). 1973.
- Sarwar R, Niclos B and Rutherford O. Changes in muscle strength, relaxation rate and fatiguability during the human menstrual cycle. J Physiol. 493: 267-272. 1996.
- Smith H, Vacek P, Johnson R, Slauterbeck J, Hashemi J, Shults S and Beynnon B. Risk Factors for Anterior Cruciate Ligament Injury. Sports Health. 4(1): 69-78. 2012
- Solomon S, Kurzer M and Calloway D. Menstrual cycle and basal metabolic rate in women. American Journal of Clinical Nutrition. 36(4): 611-616. 1982.
- Marinho A, Sallam,H, Goessens L Collins and Campbell W. Ovulation side and occurrence of mittelschmerz in spontaneous and induced ovarian cycles. Br Med J (Clin Res Ed). 284(6316): 632, 1982.
- Mesen T and Young S. Progesterone and the Luteal Phase. Obstet Gynecol Clin North Am.42(1): 135-151, 2015.
- Tenan M, Hackney A and Griffin L. Maximal force and tremor changes across the menstrual cycle. Eur J Appl Physiol. 116(1):153-60, 2016.
- Meijer G, Saris W, Westerterp K and Hoor, F. Sleeping metabolic rate in relation to body composition and the menstrual cycle. American Journal of Clinical Nutrition. 55(3):637-40, 1992.
- Blundell J. Serotonin and Appetite. Neuropharmacology. 23(12): 1537–1551, 1984.








